













Movements in the upper and lower joint
Even in complex sports movements there is no need for large amplitudes of movement in the frontal foot because the ankle is basically made to move back and forth. Movements in the other two levels are compensated for motion in the hip joint and partly in the knee when the knee joint in the half bent position.
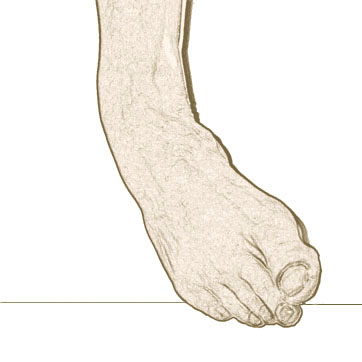
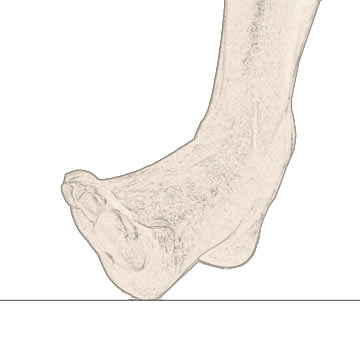
The maximum amplitude of movement in the sagittal plane (upper ankle) while movements in the other two levels are rather limited

Increased mobility causes lowering of the joint strength which increases joint injury risk
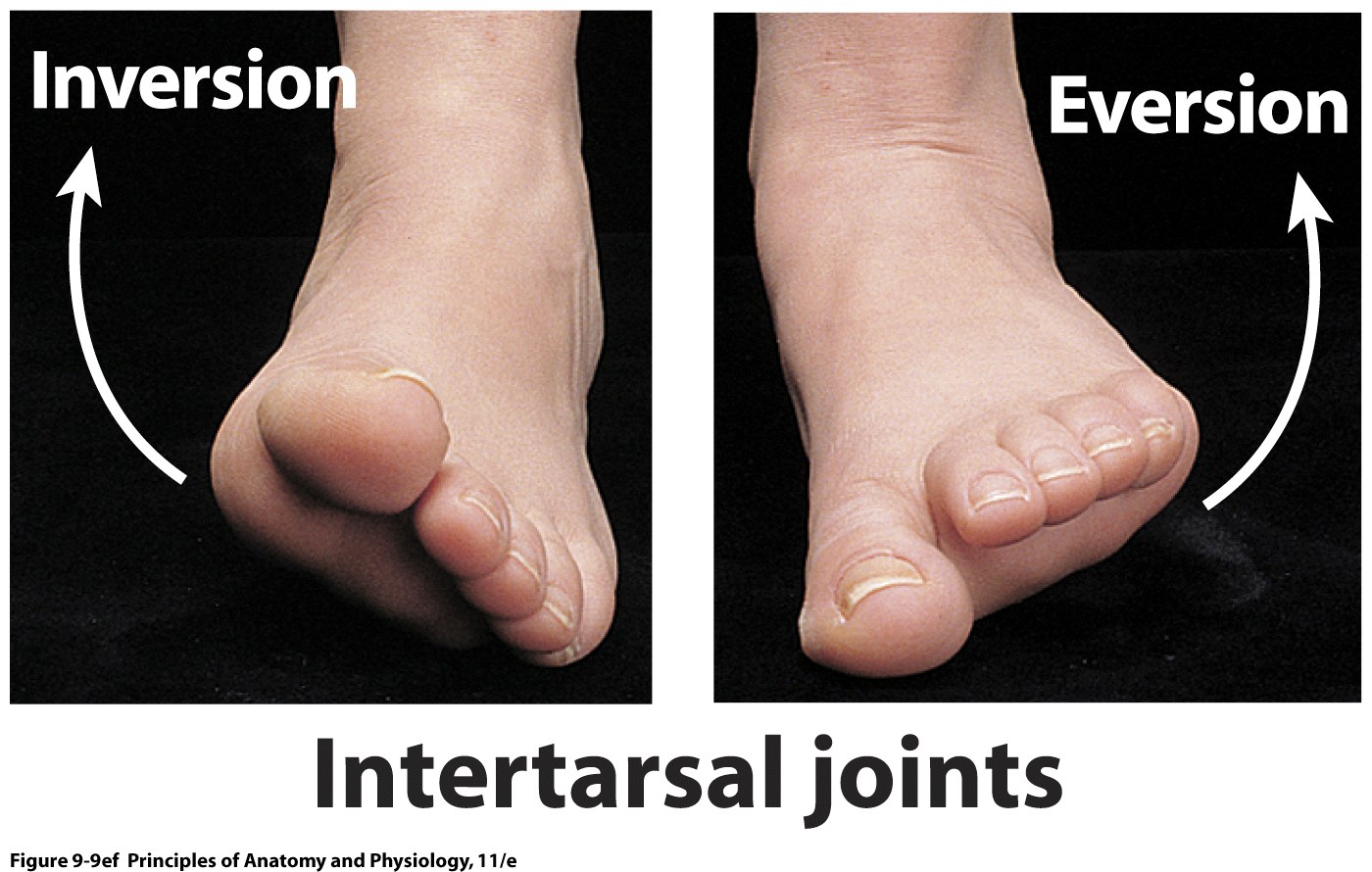
Muscle merged in the ankle are placed so that muscle contractions that start from the outside of the longitudinal axis ankle bones cause at the same time twisting and separation the foot (pes valgus), while the contraction of muscles which start on the inside of the longitudinal axis ankle bone at the same time causes distortion and bringing the foot closer (pes varus)
The function of the foot is to have stability and provide firm support for moving and its elasticity allows a suspension like effect, increased resistance when the pressure is increased, and participate in resetting (reflection) their elastic forces when the pressure is diminishing.
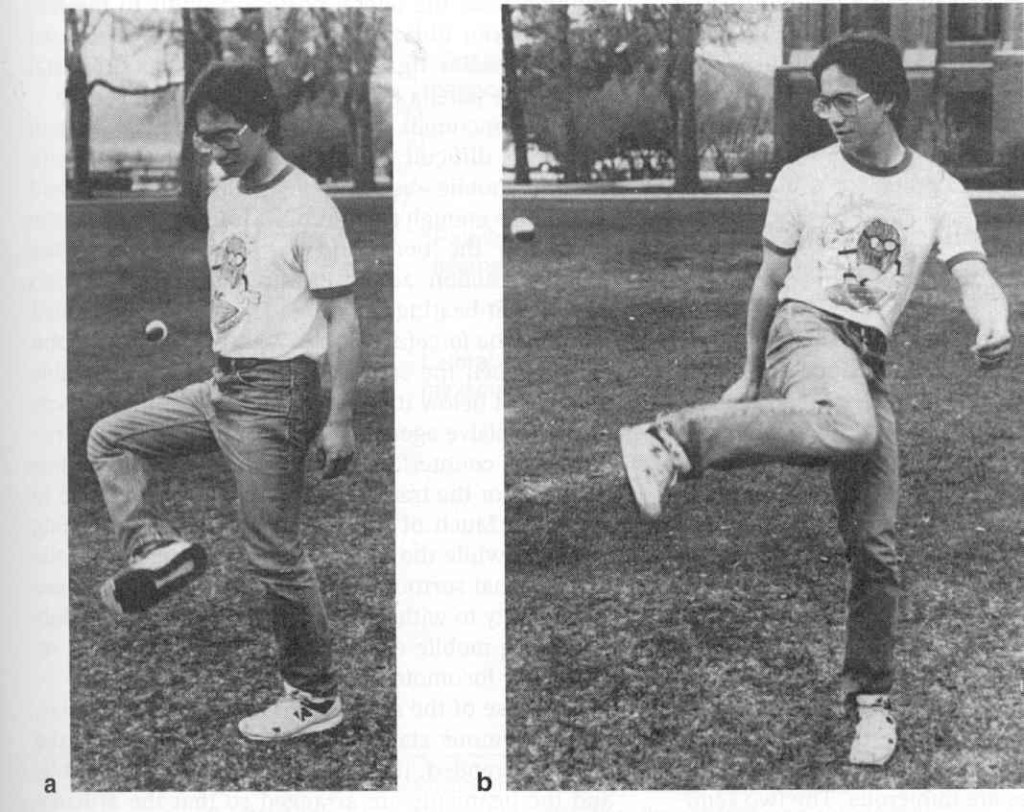
In complex movements, the human foot represents the lever of help by which we can achieve better effects in other locations (like the palm) so that in the end those extremities can create greater speed and greater resistance (eg. swimming).


FLATFOOT – HISTORY of etiology
- Whitman 1888 – inability for muscles and ligaments to keep the foot stable
- Kidner 1933. – Kidner 1933 – posture m.tibialis posterior and its attachment to the presence of tibial shaft externum that cause dynamic muscle imbalance
- Chambers 1946 – abnormal abduction of the foot beneath the talus
- Selaković 1973 – Calcaneus does not support talus
Flatfoot represents a failure or loss of the medial longitudinal arch of the foot. It may be the result of hyper pronate or increased subtalar joint eversion. Calcaneus is found in valgus position and external rotation relative to the talus.
TYPES of flatfoot
There are two types of flat feet: flexible and rigid. Rigid flat foot is very rare and it can be genetic (tarsal coalition, vertical talus) and acquired (inflammatory). On the other hand the situation with flexible flatfoot can be: development (most often), hypermobility (flexibility of ligaments) and neurogenic (rarely).
FLATFOOT pathophysiology
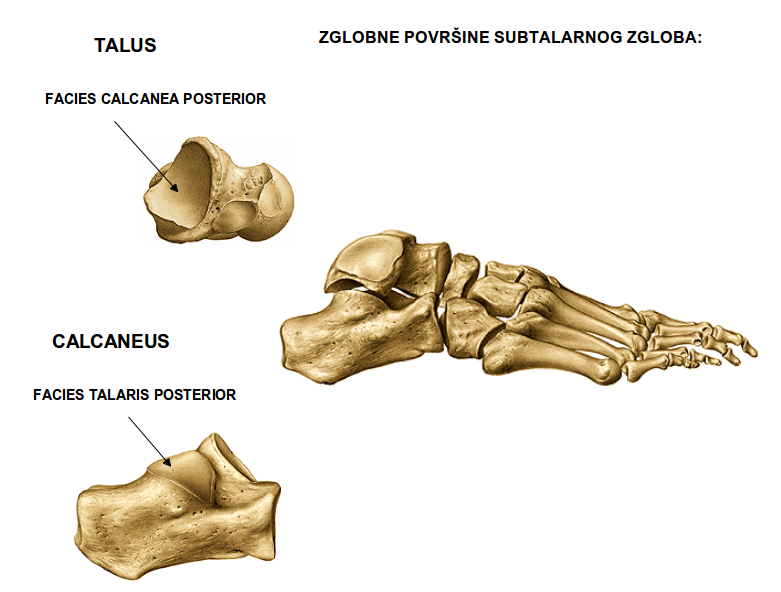
Subtalar joint is oriented obliquely relative to the axis of the ankle joint (20 ° – 57 °). The head of the talus is supported by a front extension calcaneal during eversion the calcaneus no longer supports the head of the talus, which is moved medially and plantarly, fall in the medial part of the foot which causes the inner longitudinal arch of the foot to be less pronounced.
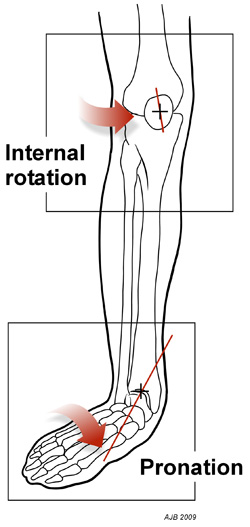
In flatfoot the shaft subtalar joint is more horizontal allowing a greater volume of inversion and eversion of the foot and lower internal and external rotation.
With flat feet longitudinal axis of the foot is moved more medially (than the normal 23 ° which allows greater plantar flexion and dorsiflexion). As a result of changes in subtalar axis leads to greater supination and pronation effects on the foot.

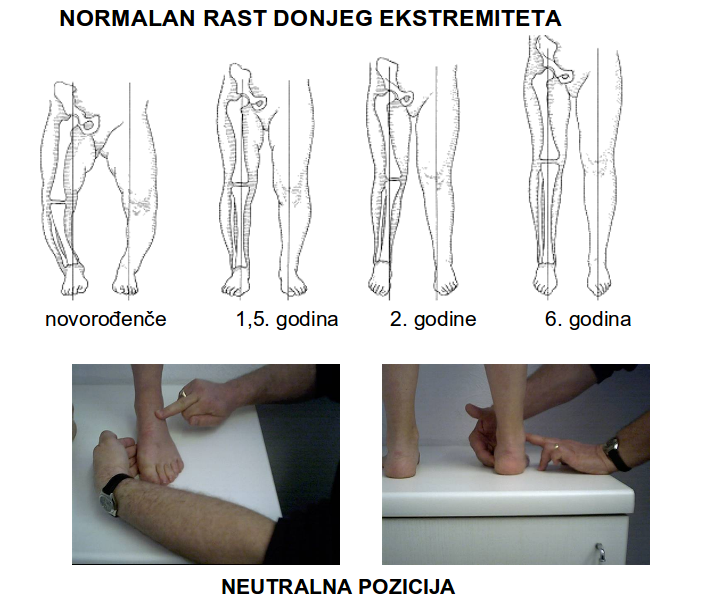
Flatfeet in children
It is normal for children who walk to have a flattening the longitudinal inner arch, pronation forefoot and heel valgus. This is due to weakness in the ligaments. Within the first decade of life, children spontaneously develop a normal arch of the foot.
Flatfeet in adults
Flatfoot in adults occurs in 20% of the population. The vast majority is of the flexible type, and vast majority will also not develop major problems.
Flatfoot with accompanying shortening of the Achilles tendon may have difficulty in walking.
Flat feet protect against metatarsal stress fractures, but are extremely weak absorbers of force and are a common cause of pain in the lower back (unlike the pes cavus).
Causes of flatfoot in adults:
- rupture tendinis musculi tibialis posterior
- defect of the calcaneonavicular ligament complex
Clinical Manifestations
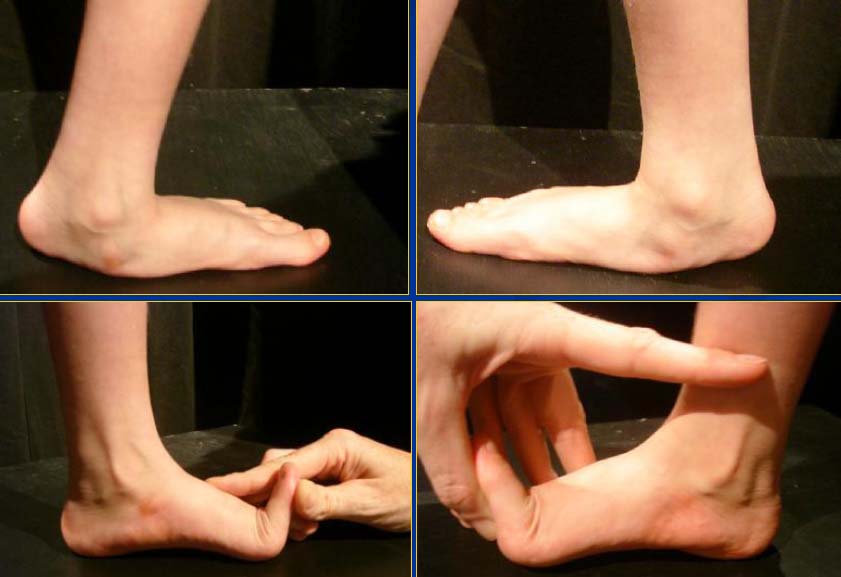
It is necessary to distinguish between the flexible flat foot and that of rigid or spastic foot!
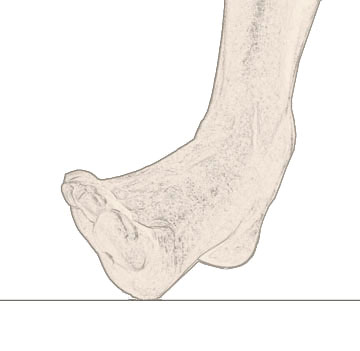
Hypermobile heel
When raising the foot again to form a normal appearance of the inner part. When standing on tiptoe internal arc re-formed and the heel moved out of valgus position into normal position.

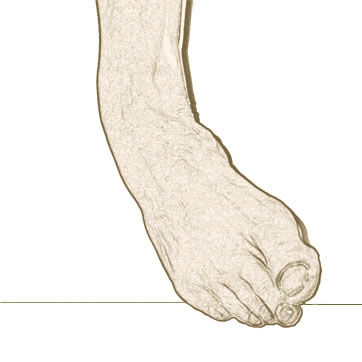
Varsus tarsa
Varus tarsusa
It is important to distinguish the collapse of the medial heel and failure m.tibialis posterior.

The medial longitudinal arch

tendo m.tibialis posterior
If the patient can stand on tiptoe on one foot m.tibialis posterior functional.
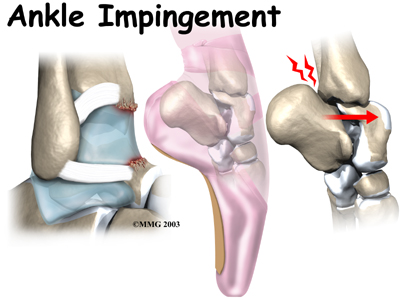
Lateral impingement (sinus tarsi i fibular calcaneal)
Contracture of the Achilles tendon
Heavy contracture of the Achilles tendon is often associated with the collapse of the inside of the foot

Hypermobile posterior heel
Abduction forefoot. Heel in eversion is not corrected when on toes.

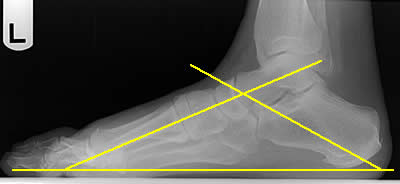
Radiographic analysis
Lateral foot x-ray while standing (increased declination talus, reduced talocalcaneal angle below 20 °, obliteration of the sinus tarsi)

Normal angle between the longitudinal axis of the talus and calcaneus is: 25° – 30°
Non-operative treatment
- The vast majority do not require treatment
- Kinesis
- Orthotics
Operative treatment -indications:
- The pain resistant to conservative therapy (tension posterior tibial nerve, tarsal tunnel sy)
- Fatigue (symptoms of overload, loss of quality of daily life)
- Degeneration of the joint (front and back of the foot)
- The joint deformities caused by flat feet (worsening deformity despite other inoperable forms of treatment, bunion, hammer toes,metatarsalgia, fasciitis plantaris, intermetatarsal neuroma)
- Cerebral paralysis
Subtalar arthrodesis:
- Chambers in 1946.
- Mechanical causes the effect of preventing hypermobility – calcaneal stop
- Proprioceptive feedback-coupled activate antagonistic muscles
- Allows remodeling in children
CLINICAL INDICATIONS FOR subtalar Arthrodesis:
- Reducible valgus posterior an aspect of the foot
- Eversion of the heel at least 8° – 10°
- Flexible tarsus varus greater than 10°
- The collapse of the inside of the foot with ptosis talonavicular joint
- paralytic foot
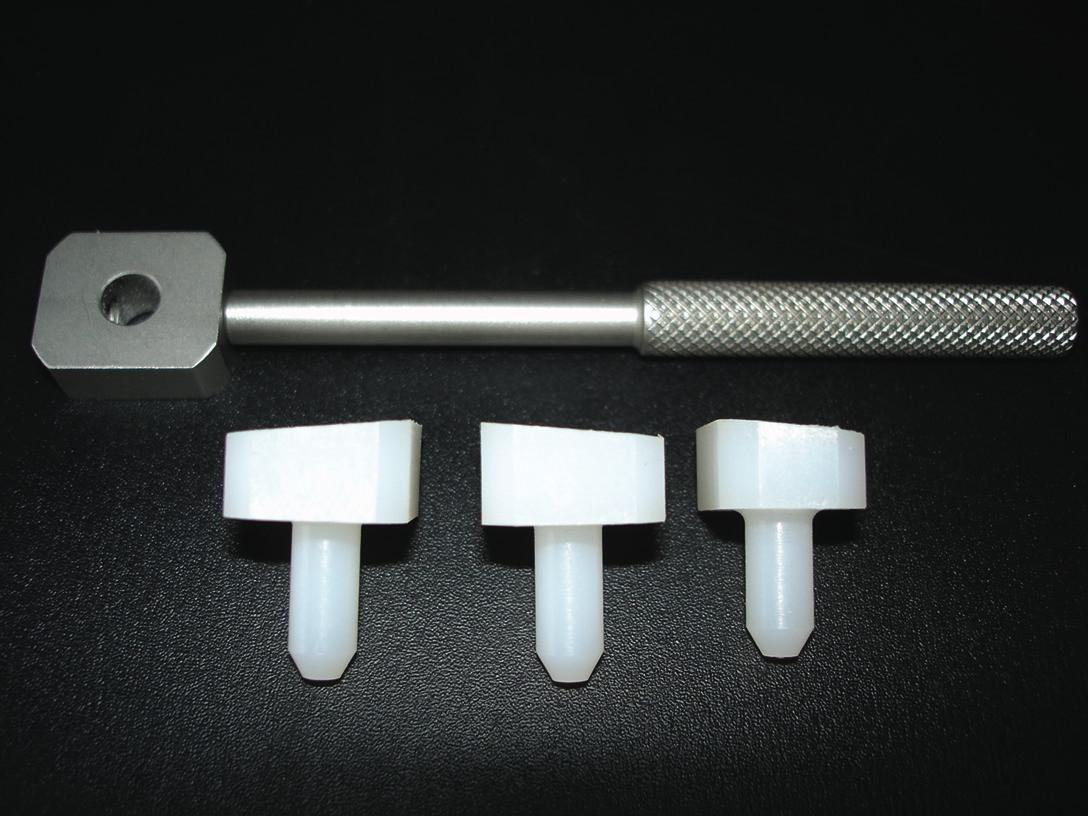
Subtalar ARTHRODESIS-IMPLANTS:
- Valgus stop prosthesis
- STA Peg
- Scaglato
- Colourful composite
- Bio absorbent
- Titanium

Implant technique:
- Postoperative foot orthoses in the supinacion wedge for 7-14 days
- Children with orthopedic shoe of the seventh day, with supination wedge and A raise of 5 mm
- Sutures are removed in 14 days
Complications:
- Excessive correction of deformities
- The reaction to the implant
- Mechanical damage to the implant
- Loosening of the implant
- Oxidisation of the bone, avascular necrosis of the talus
- Infection
- Pain
Advantages:
- Easy to perform
- Minimum patient morbidity
- One-day surgery
- It can be done under regional anesthesia
- Inexpensive instrumentation does not require special additional training-specialization
- Tertiary health care services
- The rapid return of the everyday quality of life
